
Temporo-mandibular (TM) Joint Problems and Therapy
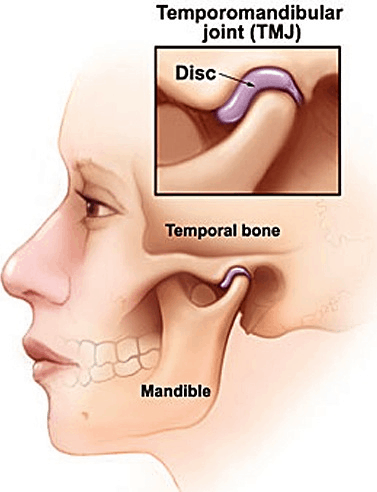
Figure 1. The TM joint has a fibro-cellular disc (partly fibrous and partly cellular) similar to a saddle that sits between the two parts of the joint (the Glenoid Fossa of the Temporal bone above and the Condyl head of the mandible below) to allow free and smooth movement of the two bones over each other.
The intra-articular disc….
This disc is designed like a saddle that sits within the joint cavity on the joint surface of the condyl head of the mandible (lower jaw). As the jaw opens so the disc moves forward with the condyl but is held in place by ligaments and tissue bands within the joint.
The joint action….
The first 2-3mm of mouth opening is the result of a “pure hinge” movement of the jaw joints. Thereafter the opening is due to a sliding action of the condyl head down the bone slope in front of the joint. This is called forward or anterior translation.
This complex movement of the TM joint is the most complex throughout all the joints in the body. We describe this movement of the TM joint as a “hinge and slide” movement.
Causes of TM joint pain….
There are many reasons why the TM joint or the associated muscles can become painful. One simple classification of TM joint disease divides the conditions into three headings.
- Myofacial Pain Dysfunction – this is described as abnormal muscular function with a wide range of symptoms with pain that can be present in a number of different patterns, often worse in the morning with individual teeth that can be sore from clenching or tooth grinding at night during sleep.
- Internal Derangement – usually damage to the fibro-cellular disc or even dislodgement of the disc from its correct position, sometimes with increased joint mobility but more commonly restricted movement of the joint and even locking of the joint frequently accompanied by a clicking sound.
- Osteoarthrosis – often accompanied by a grating noise known as crepitus. This is a disease of wear to the joint moving parts. More severe cases have bone against bone and total wearing away of the disc. This is osteoarthritis.
Trauma may damage the joint, the ligaments of the joint or the disc within the joint. Muscular injuries can be caused by trauma and can also result from disharmony between the joints, the disc and the way in which the teeth meet. However, one of the most common causes of TM joint dysfunction is a damaging habit known as clenching.
Clenching is not the same as grinding. Indeed, tooth grinding, also known as bruxism, has the effect of damaging the teeth due to severe wear, rather than the joint. Clenching however tends to damage the joint with less damage affecting the teeth. Many people clench their teeth during times of tension or stress. It is one of many stress coping mechanisms that humans use.
Clenching the teeth together uses the muscles of mastication (the chewing muscles) and has the effect of causing heavy loading of the joint, squashing the fibro-cellular disc within it. The disc is held in place by ligament tissue and with repeated heavy loads generated by clenching, these ligaments become inflamed and painful as they have a extensive nerve and blood supply.
Disc damage….
The disc can also become damaged and altered in shape by heavy loading that takes place during clenching or during trauma such as a fall. Such an injury may result in a change in disc shape or damage to those tissues that keep the disc in its correct position, on top of the condyl head. The distorted or mobile disc can then act as a mechanical obstruction to smooth movement of the joint.
Movement of the joint over the deformed or displaced disc may then lead to joint noises during movement (opening and closing the mouth and during chewing). Such noises have variously been described as jaw clicks, “cluncking”, popping or grinding (also known as crepitus). However, crepitus is usually associated with Osteoarthrosis or osteoarthritis usually accompanied by more severe and localised joint pain.
Joint imperfections can also cause sudden jerking movements of the joint, during what should be a smooth opening movement, as the disc is either trapped or freed from between the glenoid fossa and the condyl head of the mandible.
A common disc related problem is disc displacement. It occurs usually due to acute trauma, the disc is then able to move from its correct location due to damage to the soft tissue that holds it on the condyl head. Once this restraining tissue becomes loose, the disc can move independent of the condyl head.
Disc displacement most commonly occurs to a position in front of the condyl. It may return to its correct position with a click and then on opening may displace forward again with another click. We refer to this as disc displacement with reduction.
Alternatively the disc may remain displaced in the forward position causing locking of the joint or restricted opening accompanied by severe pain. We refer to this as disc displacement without reduction. The forward entrapment of the disc results in the posterior ligament or band containing nerves and blood vessels becoming placed between the condyl head and the glenoid fossa hence it become loaded during closure or clenching. This results in the band becoming inflamed, swollen and painful.
The ability of the disc to heal….
The disc is made of both fibrous tissue and a cellular component. The latter cellular tissue gives the disc its potential to heal. Healing takes time and is more effective if the joint is given a rest. Resting the TM joint is difficult however, as the joint moves all the time when we speak, when we eat and even when we sleep. This is why a soft diet is important if there is a disc injury and why a mouth splint that allows the jaw to relax is helpful in resolving any disc injury.
Muscular damage, spasm and overload….
Not all cases of TMJ dysfunction involve injury to the disc. Sometimes it is the muscles of mastication that can become tired and may be subject to small contractions that may be referred to as a spasm with the effect of the muscle becoming painful. This indicates the need for muscular relaxation to allow repair, and resupply of nutrition to the muscle fibres and the removal of chemical waste products produced in the muscle fibres when they contract. This requires rest for natural healing to take place and may be assisted by massage or manipulation of the muscles by a skilled therapist.
Muscular healing can be activated by stimulation of muscular trigger points. This is something that is outside the scope of practice of a dentist and comes into the area of expertise of a physiotherapist, remedial massage therapist or chiropractor. Depending on the nature of a patient’s problem, Dr Priestland may refer a patient to a colleague with these qualifications and a different scope of practice if he feels that a different approach is going to result in a quicker resolution of the injury.
The effects of clenching….
Clenching of the jaws frequently leads to trauma of the ligament attached to the intra-articular disc at the rear of the joint. This area of tissue has a very extensive nerve and blood vessel concentration. This trauma leads to inflammation in the tissue. One of the signs of inflammation is swelling. When swelling occurs in the posterior ligament, the ligament become painful and can become shortened due to the swelling. When the jaw opens, and the disc moves forward with the Condyl head, the posterior ligament is no longer able to stretch adequately and it tightens up restricting the disc’s forward movement. This leads to pain. Ways in which to solve this problem include restricting the loading of the joint, reducing joint activity, limiting the range of jaw opening, and prescribing non-steroidal anti-inflammatory medications to resolve the inflammation. Very occasionally muscular relaxant medication may also be required.
How to reduce clenching….
Most clenching takes place subconsciously, and also at night as part of our normal stress management. In order to eliminate or reduce this activity it is necessary to use the body’s own protection mechanism called a neuro-muscular feedback mechanism. This is best explained by considering someone chewing meat that has a piece of bone in it.
When the teeth come together heavily during chewing and they bite onto the bone fragment, immediately a message is sent through the nerve sensors in the periodontal ligament that supports the tooth, to the brain, reporting the sudden overload of the periodontal ligament. In a microsecond, the brain turns off the muscles that are closing the jaw and turns on the muscles that open the jaw, thus parting the teeth. All this happens in such a short time period that we are unaware of the reflex action. It is possible to use this naturally occurring protective reflex action to prevent clenching.
How to harness the protective reflex response….
A hard acrylic splint (hard plastic splint) is fitted to the upper teeth. This splint has a flat “bite platform” in the midline that allows the lower small incisor teeth to bite onto the acrylic but this is the only contact that exists between the upper and lower teeth. During the night, the brain initiates a clenching action and this applies all the force of loading to the small lower incisor tooth thereby overloading the nerve sensors in the periodontal ligament that supports the tooth, triggering off the protective reflex action described above. A message is then sent to the brain reporting the overload, and the brain immediately turns off the jaw closing muscles, and turns on the jaw opening muscles, and in this way stops the clenching activity taking place.
But why muscular aching….
These symptoms can be explained. Consider the upper and lower teeth clenched together. The high loading is spread across the biting surface of all the teeth and therefore the load distributed to each tooth may not be sufficient to register as an overload. Therefore the clenching muscles will not be turned off, however, the loads are fairly high and the opening muscles attempt to open the jaw. This is unsuccessful because the opening muscles are very small and relatively weak, while the clenching muscles are large and powerful. Hence the teeth remain tightly closed together while the opening muscles contract. The overall outcome of this is a tipping forward of the head and as a consequence of this movement, the muscle fibres at the back of the neck and shoulders are stretched.
Threshold electrical stimulation of muscles….
Muscle fibres must receive an electrical stimulus of a certain magnitude to contract. This electric stimulus is called the threshold stimulus. Any less, and there is no resulting muscle contraction. Any more, and the contraction remains the same and does not contract to any greater degree.
Reduced threshold of electrical stimulation….
When the muscle fibres are stretched, the threshold stimulus is reduced. This means that the muscle fibres will contract when provided with a lesser electrical stimulus.
Background electrical activity of nerves….
The nerve system is rather like a telephone exchange. Even at rest, there is a background low level of electrical activity but this level is greatly increased when the muscle is required to contract.
Muscular spasms can be explained….
At night while resting, the background level of electrical activity continues to be present, and the clenching causes the forward head tilt therefore stretching the muscles at the back of the neck and at the top of the shoulders. This stretching reduces the threshold level of electrical stimulation required to result in muscular contraction.
Now, overnight, due to the clenching action, the posterior muscles start firing off and muscle contractions begin to take place. This is often referred to as spasms. With the continued muscular activity, the muscles tire and there is a build up in the level of waste chemicals due to the muscular activity. In particular Lactic acid concentration rises and the muscles tire and become sore.
Treatment for this muscular pain….
The treatment for the soreness in the neck and shoulder muscles is therefore
- to eliminate the clenching habit and
- relax the muscles and ensure the muscles are repositioned into their normal positions.
The elimination of the clenching is the responsibility of the dentist using an appropriate splint while the correction of the muscular activity and spasms is best treated by a remedial massage therapist with a detailed knowledge of the muscular anatomy and the ability to realign the muscles and encourage their relaxation.
Arthritis
Like any joint, the TM joint can suffer from wear of the surfaces of the Temporal bone and the condyl head of the mandible. These surfaces can become pitted, abraded or smoothed so that the movement of the joint is no longer smooth and the damaged surface grinding on the opposing bone can cause pain.
In severe cases a surgical procedure may be indicated that may range from an exploratory procedure with irrigation of the joint space and then injection of steroid, to a complete replacement of the condyl head of the mandible.
This more advanced surgery is only performed by more highly specialised oral and maxillo-facial surgeons and if such severe joint disease is suspected, Dr Priestland would arrange a referral for assessment with a local oral and maxillo-facial surgeon.
Abnormalities of growth
Careful assessment of the TM joint using 3-dimensional cone beam volumetric tomography or other medical CT imaging allows visualisation of the joint to check for any unusual shape to the joint surfaces. Additional investigations may include magnetic resonance imaging for soft tissues helps to identify any unusual soft tissue growths and identify any disease that does not relate to the bone of the joint. Rarely, overgrowths of tissues found in the joint can occur that interfere with normal joint movement and function. Once again the removal of such unusual abnormal tissue would be arranged through the oral and maxillo-facial surgeon.
Contact the friendly team at NQ Surgical Dentistry today on (07) 4725 1656 or call in to see us at 183 Kings Rd, Pimlico QLD 4812

BOOK AN APPOINTMENT
CALL US TODAY 07 4725 1656