
Dental Crowns
What are crowns?
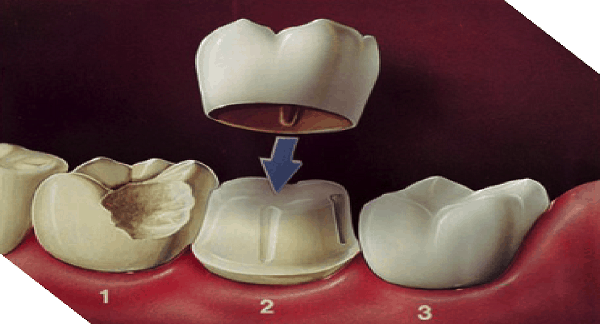
A crown is a dental restoration that can be made of various materials including metal and/or ceramic that fits over the remains of a tooth restoring its ability to function (chew), restoring it’s shape and hence providing improved appearance while strengthening the remaining tooth structure that may have been weakened either by trauma or dental decay.
Why are crowns used?
There are basically four primary reasons for using crowns:
- To strengthen a tooth when it has been attacked by dental decay. Over the years, the extent of the filling in the tooth may become so large that there is insufficient natural tooth structure remaining to provide adequate support for the filling material. The tooth has become too weak to function reliably and it can be expected to fracture under normal functional loading.
- To restore contact between upper and lower teeth to allow normal function to be re-established after extensive damage has been inflicted on teeth either by trauma (as in an accident) or from tooth wear (acid erosion with abrasion, or acid erosion with attrition – see the article on tooth wear).
- To provide an improved appearance when teeth have become a patchwork of dental fillings or when anterior teeth become badly discoloured .
- To provide a tooth like restoration on a dental implant.
What types of crowns exist?
Crowns can be divided into metal, metalo-ceramic or entirely ceramic.
Metal crowns….
The simplest of all the crowns to make are metal crowns. A skilled dental technician manufactures them from the impressions taken by the dentist. The most common metal employed for their manufacture is a specialised dental gold alloy.
Gold alone is too soft to use for full gold crowns and would not provide the right wear characteristics to last in the mouth. Constant chewing would result in the opposing teeth causing such a degree of wear to the gold that the patient would wear holes in the gold crown. In order to provide the gold with greater wear resistance and strength, very small quantities of other metals including Platinum are included in the alloy to create the ideal crown material.
Such a gold alloy can be cast at high temperature in relatively thin section to manufacture a crown. It may be cast as thin as <0.2mm and once it has been shaped to conform to the bite from the opposing tooth, the gold alloy can be polished to a very high lustre.
Other metals are also used for crowns, including stainless steel crowns for use in young children to keep the first teeth when they have become decayed and are liable to fracture. These come as an off the shelf crown to be trimmed and fitted.
Chrome cobalt crowns (non-noble metal crowns or base metal crowns) have also been used being a cheap alloy used in the provision of dentures and therefore widely available for long term provisional crowns for posterior teeth in adults. This is not common practice but can be useful when an extensive reconstruction of damaged teeth is to be provided over an extended period of time and these crowns prevent tooth movement and protect the remaining tooth structure but the crowns do not wear themselves.
Gold is considered very acceptable in the teeth in some cultures but not all. Increasingly over the past decades, patients have requested that crowns appear as near as possible like natural teeth. This “market driven desire” led to the use of porcelain as a dental restorative material. However, porcelain is extremely brittle, especially when used in thin section. In order to make crowns appear natural while being strong enough to withstand the functional loads generated in the mouth during chewing, two layer-crowns called a metalo-ceramic crowns were developed. These are a combination of a metal substructure to provide strength and a surface layer of aesthetic porcelain (Feldspathic porcelain) to provide the natural tooth coloured appearance.
Metalo-ceramic crowns, also known as bonded porcelain crowns (BPCs)
These use a sub-structure of modified dental gold “bonding” alloy with a significant content of other non-precious metals that allow a surface oxide layer to develop. It is to this oxide layer that the porcelain bonds when it is fired in a high temperature dental furnace. The porcelain has an underlying opaque layer to cover the metal in order to hide the dark colour and prevent a shadow showing through the surface porcelain. The only problem with this is that such crowns may have tooth colour but have no translucency (the ability to transmit light through them) and therefore they appear somewhat flat and lifeless. This explains why such crowns are commonly used in the back of the mouth where they are less obvious.
While the benefit of combining the strength of metal and the aesthetics of ceramic is better appearance than metal alone, the “biological cost” of such a combination is that the crown must be thicker to accommodate the two materials. As a consequence, a greater thickness of natural tooth and filling material must be removed from the tooth to make room for the metal and porcelain layers of the crown. Hence the tooth preparation for a BPC is more destructive of the tooth structure than a purely metal crown preparation, hence the term “biological cost”.
The greater tooth preparation is sometimes followed by a greater degree of tooth sensitivity after the tooth has been prepared. This is due to the large amount of tooth dentine that has been drilled. The damage caused by the drill can sometimes lead to inflammation in the pulp of the tooth and in some cases the inflammation can become irreversible leading to the death of the tissues within the pulp. Once the tooth is dead it can become infected and a dental abscess may form.
From the previous paragraph, the moral of the story is that teeth should receive the least preparation possible if the preparation itself is to leave the tooth healthy and not cause additional problems.
With the current level of clinical knowledge and the availability of modern dental materials, it is not common at NQ Surgical Dentistry to provide a metalo-ceramic crowns/BPC’s any longer. There are usually strong, aesthetic and acceptable alternatives that retain far more natural tooth tissue thereby minimising the biological cost or tooth preparation.
A further problem that can arise when using BPCs is that the porcelain to metal oxide bond can fail and the porcelain can chip off the underlying metal sub-structure leaving a rough surface that can cause trauma to the soft tissues, and the rough exposed and unglazed porcelain can then act as sand paper causing severe wear to the tooth it bites against in the opposing jaw.
Metalo-ceramic crowns have been in use for around 50”. Many dentists who used to place only gold crowns in the posterior chewing teeth changed to use these BPCs due to the market driven desire to have teeth repaired with materials that looked like the original tooth. However nowadays there are a number of tooth coloured crown materials that provide high strength combined with excellent appearance including, in some materials, a reasonable degree of translucency.
Ceramic crowns….
Ceramic crowns called porcelain jacket crowns (PJCs) were used for many years as crowns in the anterior part of the mouth where appearance was of great importance. However, being ceramic they were brittle and any trauma to this area would invariably lead to their fracture.
With time and research, stronger ceramic crown materials that did not require a metal sub-layer, as in BPCs, were developed. The benefit of eliminating the metal was that there was no longer a need for an opaquer to hide the underlying metal and therefore the translucency of the crown was far greater with improved appearance.
The poor physical properties of the early ceramic crowns (PJCs) was overcome by using various materials other than metal as a core material beneath aesthetic porcelain to provide strength and good appearance in the same way as the metal did for BPCs.
Alumina crowns….
Alumina was first used in 1989 and then the outer visible surface was built up in Feldspathic porcelain providing good appearance. These crowns provided more resistance to fracture and were widely used through the 1980s and 1990s.
Empress crowns….
Another material used to improve strength and achieve excellent appearance is Leucite. This is used in “Empress crowns” to reinforce the ceramic and to create a pressure injected ceramic with superior physical properties.
Zirconia crowns….
Zirconia was then used to provide a strong substructure with Feldspathic porcelain built up over it to create a highly aesthetic crown.
In any crown that has been provided in layers with a porcelain build-up on a substructure, there is a point of weakness at the joint between the outer porcelain and substructure material beneath. This is the reason for the development of a single-phase material that possesses high strength and good appearance. The first generation of such materials is now in use called monolithic zirconia..
Monolithic Zirconia….
This material is provided as a single-phase ceramic block that can be milled into any shape. This is used in conjunction with CAD/CAM systems (computer added design/computer aided manufacture) that are now appearing in many dental surgeries and dental laboratories.
The dentist simply scans the teeth with a 3D-scanner, and the image data is either sent to a dental CAD/CAM laboratory or is passed into a milling machine on site in the dental practice.
The software in the milling machine then drives the mechanical milling machine to shape the block creating a crown that fits the scanned tooth made of a single-phase ceramic material of great strength and having no weak junction between layers of different materials.
The main problem with monolithic zirconia crowns is that translucency is not of a high level and therefore these crowns have a poorer appearance than Feldspathic porcelain over a non-metalic sub-structure. As a result few dentists choose to use monolithic zirconia crowns in the aesthetic zone at the front of the mouth, preferring to restrict their use to the back teeth where they are less obvious.
The main benefit of the dentist having the scanner and milling machine on site is that the crown can be fitted after a very short period of time (around 30 minutes) rather than requiring a patient to return a couple of weeks later for fitting. It also eliminates the need for a temporary crown made from a plastic or resin to protect the tooth over the period until the final crown returns from the laboratory. Such CAD/CAM machines are very expensive costing over Aus$100K. Such an investment is only practical in a practice that has either multiple dentists operating, or where a dentist’s main work involves the provision of crowns, as in a specialist prosthodontist practice.
Many dentists prefer to take their own impressions of the prepared teeth and pass them to their own dental technician who pours the dental stone models. These models are then sent to a specialised CAD/CAM dental laboratory for scanning and for the crown to be milled. The milled crown can then be finished and polished and returned to the dentist for fitting.
SUMMARY
- The choice of the type of crown is a technical one and patient’s are best guided by their dentist as the decision depends on a number of technical factors including:
- location of the tooth in the mouth,
- aesthetic demands (need for excellent appearance)
- relationship of upper and lower teeth,
- habits such as tooth grinding,
- degree of previous tooth destruction,
- space available between the gum and the position of the biting surface of the tooth.
There are certain situations where crowns are strongly advised. The most common and accepted indication for a crown is where a tooth has a root filling. The procedure of carrying out the root filling involves removal of a significant quantity of internal dentine from the root canals leaving the tooth weaker. Such teeth often fracture after a relatively short period of time in service. Therefore root filled teeth are definitely best crowned in such a way as to strengthen the remaining tooth structure with the aim of preventing tooth fracture and preserving the tooth for a longer period of time.
In certain cases, patients may be dissatisfied with the appearance of their front teeth. This may cause the patient some degree of distress and lead to self-consciousness. This may be due to:
- discoloured teeth,
- heavily filled and stained fillings in front teeth,
- poorly shaped teeth,
- the presence of spaces between the teeth, or
- missing teeth.
In such cases the dentist may discuss the various options, costs, and all the pros and cons of each option to make sure that the patient is receiving the treatment most suitable for them. No single treatment is right for everyone and this is the reason why such treatment planning must be performed only after a thorough examination and assessment with discussion with the patient of what they want and what they can afford..
Contact the friendly team at NQ Surgical Dentistry today on (07) 4725 1656 or call in to see us at 183 Kings Rd, Pimlico QLD 4812

BOOK AN APPOINTMENT
CALL US TODAY 07 4725 1656